Patients
-
- Angiography
- Angioplasty and Stenting
- Aortic Aneurysms
- Biliary Drainage and Stenting
- Carotid Artery Stenting
- Central Venous Access
- Colonic Stenting
- Fibroids
- Gastrointestinal Haemorrhage
- Gastrostomy
- Hepatic Malignancies
- Kidney Tumour Ablation
- Minimally Invasive Treatments for Vascular Disease
- Nephrostomy
- Oesophageal Stents
- Pelvic Venous Congestion Syndrome
- Percutaneous Nephrolithotomy
- Prostate Artery Embolisation PAE
- Pulmonary Arteriovenous Malformations
- PAE Patient Information Leaflet
- Ureteric Stenting
- Varicoceles
- Varicose Veins
- Vascular Malformations
- Vertebral Compression Fractures
- Vertebroplasty and Kyphoplasty
Oesophageal Stents
Content by Dr Jane Phillips-Hughes, Consultant Interventional Radiologist, John Radcliffe Hospital, Oxford.
Contents |
What are oesophageal stents?
 The oesophagus or gullet is a hollow muscular tube which takes food from the mouth down to the stomach. If the oesophagus becomes narrowed or becomes blocked, swallowing and eating can be difficult. One way of overcoming this problem is to insert a metal mesh tube called a stent across the blockage.
The oesophagus or gullet is a hollow muscular tube which takes food from the mouth down to the stomach. If the oesophagus becomes narrowed or becomes blocked, swallowing and eating can be difficult. One way of overcoming this problem is to insert a metal mesh tube called a stent across the blockage.
What do stents look like?
A variety of stents are available, they are made of a flexiblemetal mesh, and most have a plastic coating. In some designs the plastic covering extends over the end of the stent to produce an “anti-reflux valve”. Prior to insertion they are mounted on a long introducer catheter, similar in diameter to a ball point pen, and constrained by an overlying plastic cover or sheath.
Once in position, the overlying sheath is gradually pulled back and the stent opens up (“self-expands”) to a diameter in the region of 18-26mm. Stents of different lengths are available, but most are around 10-12 cms long. The length of and width of the stent inserted is chosen to match the length of the stricture and size of the patient’s oesophagus.
When are oesophageal stents used?
 Most oesophageal stents are inserted for strictures caused by malignant tumours involving the oesophagus, and the diagnosis will have been made beforehand by endoscopy, and perhaps a barium study and /or CT scan.
Most oesophageal stents are inserted for strictures caused by malignant tumours involving the oesophagus, and the diagnosis will have been made beforehand by endoscopy, and perhaps a barium study and /or CT scan.
A stent may be used either as definitive treatment, or it may be used to improve the patient’s swallowing whilst other treatments such as surgery or radiotherapy are planned.
Occasionally tears in the oesophagus can develop, either spontaneously, during certain procedures such as endoscopy, or if a tumour from the airway grows into the oesophagus. Stents can then be used to cover the affected area and seal the “leak”.
Also, temporary or “removable” stents are also sometimes used to treat benign strictures in the oesophagus, with the stent being removed after a few weeks / months.
The procedure
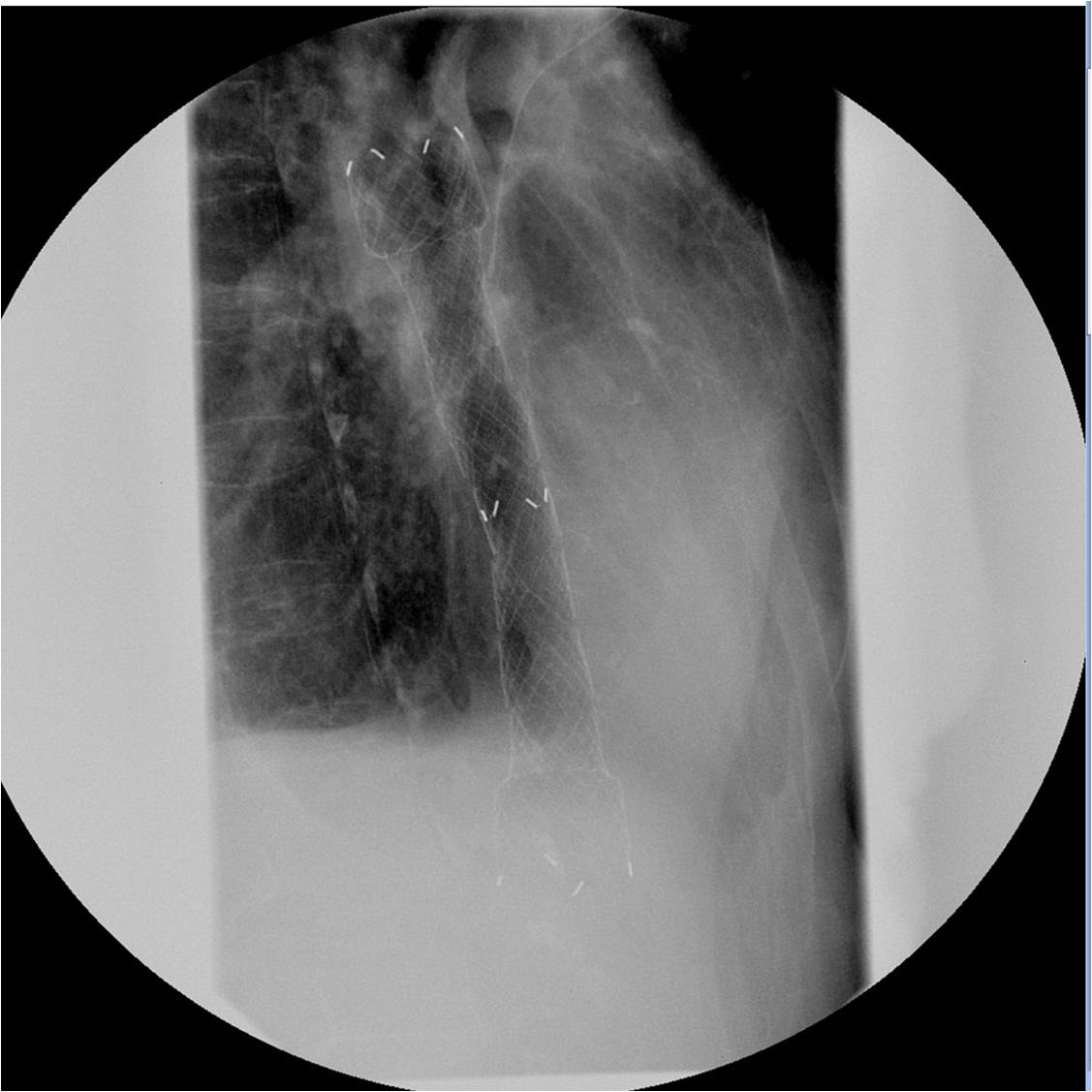
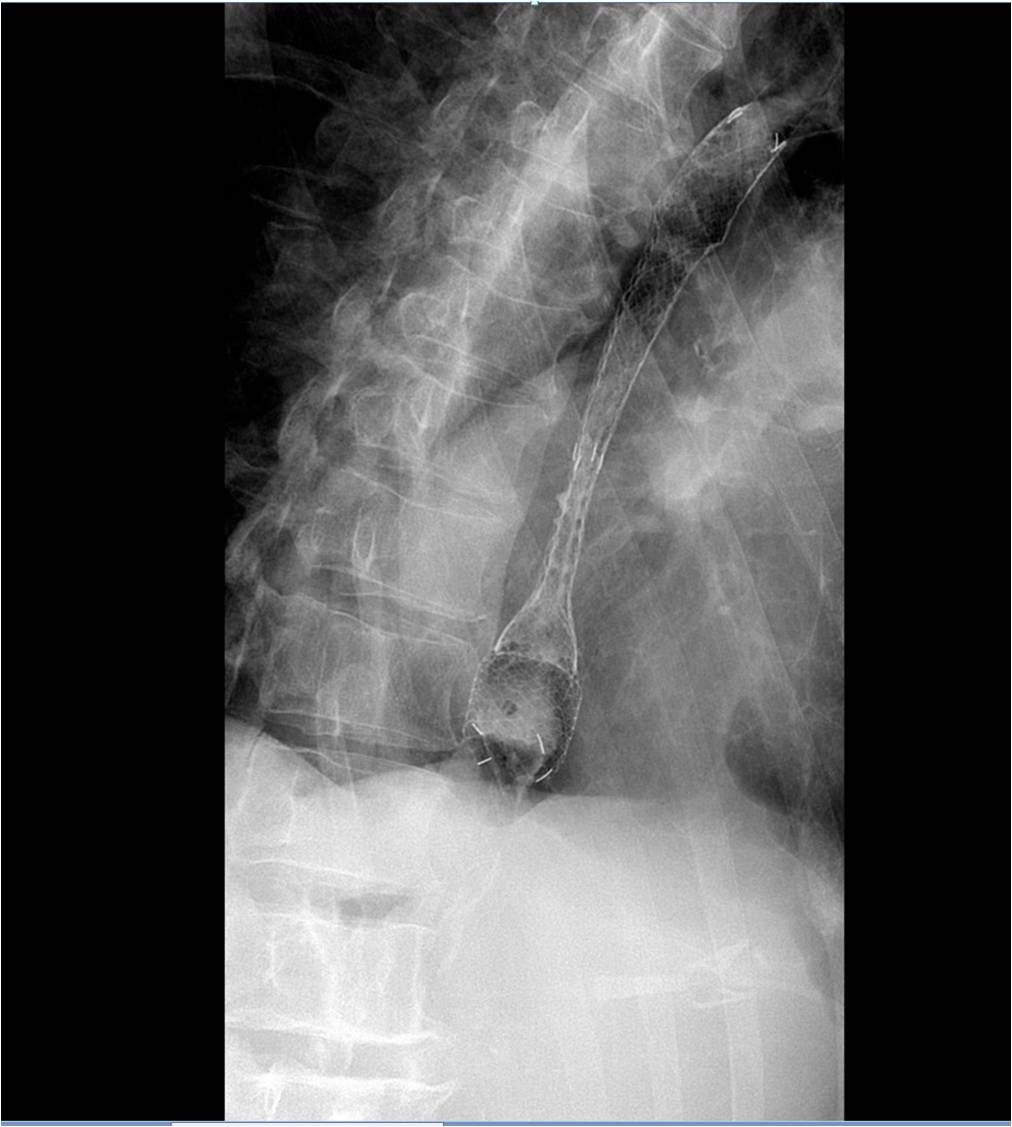
The procedure generally takes around 20 mins, but can be a little longer, and is performed under intravenous sedation. A local anaesthetic throat spray may also be used to numb the back of the mouth. A fine tube (catheter) or an endoscope will be introduced through the mouth, and into the oesophagus (gullet) and then the stricture is crossed with a guidewire using either x-rays or endoscopic vision as guidance. Once the wire is safely across the stricture the stent mounted on a delivery system is passed over the wire and once in a satisfactory position, the stent is released and will begin to gently expand.
Oesophageal stent insertion generally requires at least one overnight stay in hospital, with the patient being discharged once eating and drinking comfortably.
Complications
Stent insertion is generally a safe, simple and effective procedure, but as with all medical treatments there are some risks:
Minor bleeding may occur, but this generally stops without any need for further treatment.
Occasionally the stent may slip out of position and the procedure may need to be repeated.
Very rarely, a tear can develop in the oesophagus during stent insertion. This is a serious complication that may require an operation or another stent insertion.
In time, some tumours grow and block the ends of the stent, in which case a further stent insertion may become necessary.
Side effects
It is not unusual to feel mild to moderate chest pain for a day or two following the procedure, but the body usually adapts to the stent quite quickly, and simple painkillers will usually suffice. Occasionally stronger intravenous painkillers may be required for a short time.
Some people get heartburn or acid reflux afterwards, but again this is usually controlled by simple measures or medication.
After an oesophageal stent has been inserted
It is advisable to begin by eating liquidised meals, and then move on to a soft diet before gradually introducing more solid foods. These should be chewed thoroughly before swallowing. A dietician should be available locally to give further advice on appropriate foods.
To help prevent food sticking and possibly blocking the stent, drink regular sips of fluid with whilst eating, although avoid filling up on drinks at he expense of food. If the stent seems to be blocked then try standing up and taking sips of fluid. Warm or fizzy drinks may help clear a blockage. If the blockage does not clear then seek medical advice.
New and future treatments
Temporary (dissolving) stents are now available and are being used in the treatment of some benign oesophageal strictures that are refractory to conventional treatments such as balloon dilatation. (Ref Stivaros et al below)
Self expanding stents are also now in use for the treatment of complicated variceal haemorrhage. (Ref Wright et al below and NICE guidance link).
Cost (NHS tariff and typical private range)
The cost of a stent varies but is usually somewhere in the range of £600-800.
NHS Tariff / HRG code varies depending on method of insertion, but the tariffs are currently £489.00 for radiological insertion and £691.00 - £1013.00 for endoscopic insertion. This is due for review in 2011.
References and further reading
Quality improvement guidelines for placement of oesophageal stents. Sabharwal T, Morales JP, Irani FG, Adam A; CIRSE:Cardiovasc Intervent Radiol. 2005 May-June;28(3):284-8.
Interventions for dysphagia in oesophageal cancer. Sreedharan A, Harris K, Crellin A, Forman D, Everett SM Cochrane Database Syst Rev.2009 Oct7;(4):CD005048.
Role of oesophageal stents in benign and malignant diseases. Sharma P, Kozarek R. Practice Parameters Committee of American College of Gastroenterologists.Am J Gastroenterol. 2010(Feb);105(2):258-73.
Woven polydioxane biodegradable stents: a new treatment option for benign and malignant oesophageal strictures. Stivaros SM, Williams LR, Senger L, Wilbraham L, Laasch HU. Eur Radiol 2010 May;20(5):1069-72.
A self-expanding metal stent for complicated variceal hemorrhage: experience at a single centre. Wright G, Lewis H, Hogan B, Burroughs A, Patch D, O’Beirne J. Gastro Intest Endosc. 2010 Jan:71(1):71-8.
Links
Patient information leaflets may be downloaded from: