Patients
-
- Angiography
- Angioplasty and Stenting
- Aortic Aneurysms
- Biliary Drainage and Stenting
- Carotid Artery Stenting
- Central Venous Access
- Colonic Stenting
- Fibroids
- Gastrointestinal Haemorrhage
- Gastrostomy
- Hepatic Malignancies
- Kidney Tumour Ablation
- Minimally Invasive Treatments for Vascular Disease
- Nephrostomy
- Oesophageal Stents
- Pelvic Venous Congestion Syndrome
- Percutaneous Nephrolithotomy
- Prostate Artery Embolisation PAE
- Pulmonary Arteriovenous Malformations
- PAE Patient Information Leaflet
- Ureteric Stenting
- Varicoceles
- Varicose Veins
- Vascular Malformations
- Vertebral Compression Fractures
- Vertebroplasty and Kyphoplasty
Nephrostomy
Content by Dr Sivanathan Chandramohan, Consultant Interventional Radiologist, and Dr Andy Christie, Gartnavel General Hospital, Glasgow.
Contents |
What is a nephrostomy?
Firstly, by simply translating this medical term we gain a better understanding of what it means:
Nephros - from the Greek kidney
ostomy - forming a new opening for the elimination of bodily waste.
 The waste we are referring to is urine, which is normally drained from the kidney via the bladder. A nephrostomy creates an artificial opening in your kidney to allow urine to be drained by a different route. This involves placing a catheter (a thin tube about 30 cm in length) from the kidney to exit from the skin surface overlying your kidney. You may be familiar with the term catheter, which usually refers to draining urine from the bladder to an external bag. The catheter used in this case is very similar, and will also involve a draining bag which will be attached to your back or leg.
The waste we are referring to is urine, which is normally drained from the kidney via the bladder. A nephrostomy creates an artificial opening in your kidney to allow urine to be drained by a different route. This involves placing a catheter (a thin tube about 30 cm in length) from the kidney to exit from the skin surface overlying your kidney. You may be familiar with the term catheter, which usually refers to draining urine from the bladder to an external bag. The catheter used in this case is very similar, and will also involve a draining bag which will be attached to your back or leg.
Nephrostomy is a common interventional procedure which is performed by Interventional Radiologists or Radiologists with a Urology interest. It is undertaken in most Radiology departments in substantial numbers. Circle shows the site of exit on the skin surface of a right kidney nephrostomy catheter.
Location and Function of the kidney
Knowing the basics of the anatomy and function of the kidney will aid your appreciation of the chapters which follow.
They are positioned just behind the lower aspect of our rib cage, at the back. The right one is closely related to the liver, and the left to the spleen. Parts of our bowel (or digestive tract) also tend to be close by. The length of the adult kidney is 8-11cm, weighing approximately 120 grams.
Kidneys are essential for our survival. This importance is highlighted by the fact that despite their small proportion (about 0.5% of your total body weight), they receive around 15% of the total blood volume that is pumped out of the heart. Most of us have two, but many people manage normally with just one. Indeed, many people will be completely unaware that they have one missing. Our capacity to cope with only one is the reason why people are able to be kidney donors.
One of their main functions is producing urine to be eliminated from the body. However, they also perform several other very important tasks, which is why they are essential to our existence. For example, they aid in blood pressure control and maintaining the composition of the chemicals in our body. It is worth knowing that we are made of as much as 70% water, which contains numerous chemicals.
It is in the regulation of our chemical make- up that urine is largely produced. The kidney acts by sieving out the unwanted fluid and chemicals. The urine first collects in a structure called the pelvis (see image 5 in chapter How are my blocked kidney(s) diagnosed?). It then enters the ureter (see image 8 in chapter Performing the procedure) to be stored in the bladder, before finally being expelled via the urethra.
Why do I need a Nephrostomy?
As outlined previously, there is a pathway for urine to enter the bladder from the kidney collecting system. If this route becomes obstructed at any part, then a nephrostomy can offer an alternative means for urinary excretion.
Because the flow is being blocked, this causes the urine collecting part of the kidney (the pelvis- see the previous chapter) to dilate. This is termed hydronephrosis. The resultant back pressure leads to progressive kidney damage and deterioration of function.
There are various conditions which can result in an obstruction to urinary flow.
Not all of these will be relevant to you.
The doctors in charge of your care will be able to explain the reason why you are having the procedure in advance of it being performed.
Almost every patient is treated on an inpatient basis. Many of the indications require that the procedure is performed within a few days to prevent permanent kidney damage. Partly because the obstructed urine is stagnant, it can become infected with bacteria, which can spill into the bloodstream resulting in sepsis. These patients require the nephrostomy to be performed urgently.
Indications:
- Urinary obstruction secondary to stones (calculi), or benign strictures.
- Obstruction caused by tumours. This can be from tumours of the renal pelvis or ureter itself, or from external compression. This is most commonly seen with cancers from pelvic region.
- To divert the urine from the renal collecting system in an attempt to heal fistulas. These are abnormal communications between the collecting system and other structures e.g. bowel, vagina.
- Treatment of urinary tract obstruction related to pregnancy.
- Treatment of complications related to renal transplants.
- Access for other procedures e.g. ureteral stent placement and stone retrieval.
How are my blocked kidney(s) diagnosed?
Patients that require a nephrostomy are almost always already inpatients. There are routine tests that are performed on nearly all patients that are admitted to a hospital ward. The results of these can indicate to the doctors looking after your care that your kidneys are not performing normally. For example, because the flow of your urine in blocked, the amount that you are producing will reduce, or you may not be passing urine at all. Also, certain chemicals in your blood are very sensitive at indicating deterioration in your kidney function.
A request will be made to the Radiology department at the hospital for a scan of your kidneys. Sometimes, however, the problem is detected when your kidneys are included on a scan which is being performed for a different reason.
Ultrasound and computed tomography (CT) are the scans which routinely diagnose hydronephrosis (blocked kidneys).
Ultrasound:
This is a completely harmless test which uses sound waves to create images of the inside of your body. It is best known for its use in scanning pregnant women.
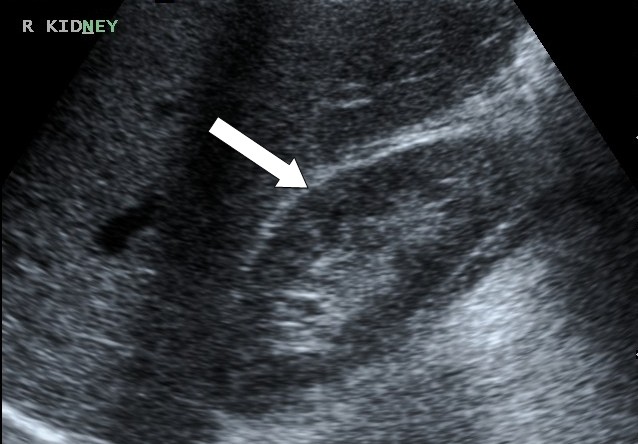 Ultrasound scan of a normal kidney.
Ultrasound scan of a normal kidney.
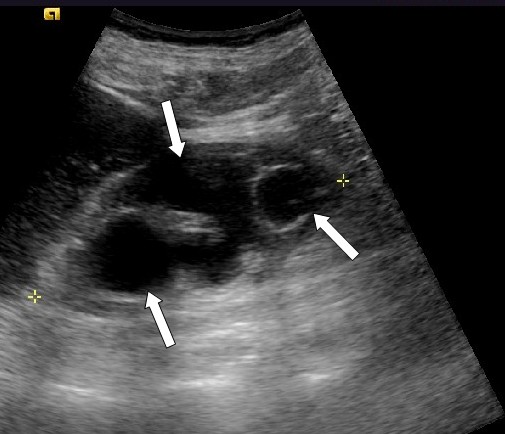 Ultrasound of a kidney showing dilation of the urine collecting system (arrows). The kidney is hydronephrotic.
Ultrasound of a kidney showing dilation of the urine collecting system (arrows). The kidney is hydronephrotic.
Computed Tomography:
This is a very sophisticated X- ray scanner which has become one of the main pieces of equipment in all Radiology departments in helping to diagnose a vast range of conditions. It does require subjecting you to radiation. However we all receive natural background radiation in our everyday lives. The radiation from a CT of the abdomen and pelvis is equivalent to about 4.5 years of background radiation.
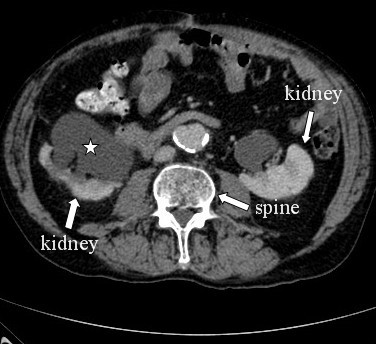
A CT scan. The asterisk shows the dilated kidney collecting system, also called the pelvis.
It is important that you realise that we do not subject you to this test unless the benefits to your care outweigh this additional radiation.
Is there an alternative treatment?
Certain surgical procedures can be used, particularly when more permanent diversion is required. Urology specialist doctors can place tube between the bladder and the kidney, called a ureteric stent. This involves placing a camera into the bladder from below, which is usually done under general anaesthesia but occasionally performed under sedation and local analgesia. In the acute setting in particular, a nephrostomy is preferred to more invasive alternatives as it is less likely to cause overwhelming infection, the consequences of which can be very serious.
There are very few contraindications to the procedure:
- Bleeding disorders- in particular an inability to form clots to stop bleeding.
- Uncooperative patient.
- High levels of the chemical potassium in the blood (hyperkalaemia). This should be corrected with haemodialysis before the procedure.
Performing the procedure
Once the problem with your kidney(s) has been diagnosed, the doctors in charge of your care will discuss your case with an Interventional Radiologist, who will perform the procedure.
As previously described, the procedure is then performed relatively urgently, usually within 1 to 3 days, depending upon your individual case. This allows you some time to discuss any concerns.
Informed consent is always taken from the patient. Rarely, patients are too sick to be able to give consent themselves. This can happen for a variety of reasons. In this situation, the doctor can still proceed if it is deemed to be in your best interests.
The procedure is carried out in the X- ray department utilising X- rays to allow real time imaging (known as fluoroscopy). The room resembles an operating theatre and can be intimidating. This is however necessary to prevent any possible spread of infection, and you need not be alarmed.

Example of inside of an interventional radiology theatre where the procedure occurs.
The patient lies down on the X- ray table, on their front. A doctor or nurse may inject painkillers or sedation via the cannula in your vein, but this is usually not required. Antiseptic cleaning solution is applied to the skin over the kidney, and sterile drapes placed around this site. Local anaesthetic is injected into the skin over your kidney. This is often the part of the procedure that causes most pain. It is similar to the jag that dentists use, and should be numb after a few minutes. You will still be aware of the area being touched throughout the procedure, but it shouldn’t be painful. If it is, you should inform the nurse or doctor.
Your pulse, heart rate, oxygen level and blood pressure are monitored constantly with special equipment.
Before starting to place the nephrostomy, the doctor will use a portable ultrasound machine to make a final check on the obstructed kidney, and to decide where to place the catheter within the kidney. A series of guide wires and catheters are then used to gain access to the kidney. All this is guided with X- ray and contrast dye to help provide images. You might hear the word “dilator” being mentioned. This is another type of catheter that helps create the artificial tract to the skin surface. Patients often feel pressure or mild discomfort at this stage- but it shouldn’t be painful.
Once the catheter is in place, it will be exiting from the skin over the kidney. Urine will then pass down the tube into a bag which will be attached.
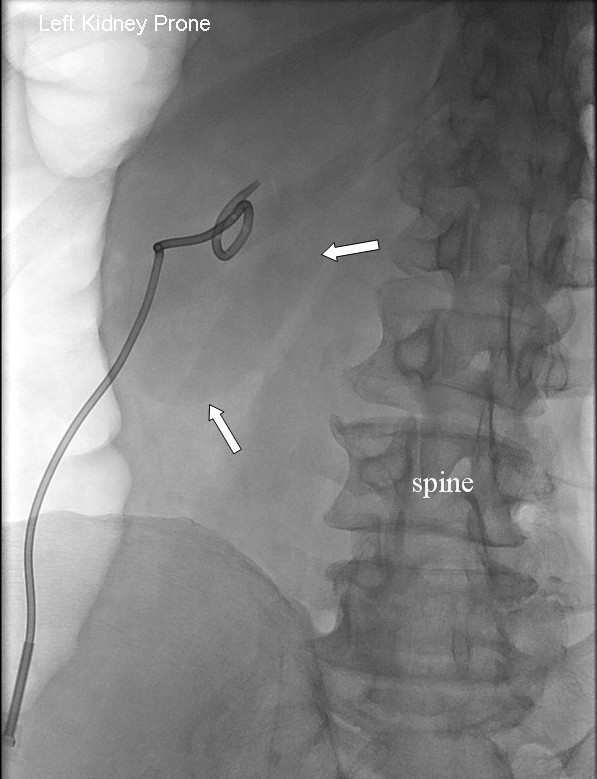
Image taken during the procedure showing the nephrostomy catheter within the patient’s left kidney. The arrows point to the outline of the kidney.
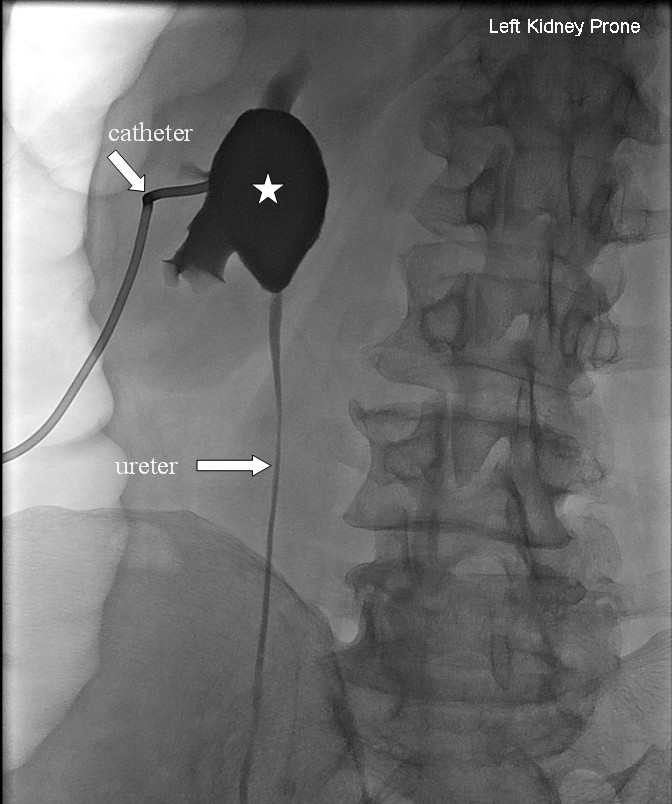
Image taken during the procedure shows x-ray dye(contrast) outlining the dilated kidney (asterisk). Contrast is also outlining the ureter which then drains into the bladder.
The procedure takes about 30 minutes. But every case is different, and your kidney might prove difficult to gain access to. This will inevitably prolong the procedure, but it should not alarm you.
What happens after the procedure?
You will be returned to the ward as soon as the procedure is finished, and it is safe for you to be transferred. It is perfectly normal for you to require further pain relief for a day or two. Also, most patients will pass some blood in the urine for a few days which is again to be expected.
There is no defined time for when the nephrostomy should be removed as every patient’s case is unique. You will have regular blood checks and possibly further ultrasounds/ CT scans to help decide upon this. You may even have to have the catheter exchanged for a new one before it is finally removed. A catheter has a life span of approximately 3 months. It is replaced to prevent occlusion and to reduce infection risk.
If you require a nephrostomy on your other kidney. This can be performed at the same time, or at a later stage.
In certain circumstances, the nephrostomy is placed in advance of a ureteric stent. This can be inserted immediately after the nephrostomy. Sometimes a few days of drainage via the nephrostomy catheter are required before hand. This decision is made if there is pus within the urine, or the collecting system is grossly distended making it technically difficult to access the bladder.
Complications
In 2004, the Royal College of Radiologists and the British Society of Interventional Radiologists created a UK National Nephrostomy Register to compare our practice outcomes with others. This has shown that our standard is satisfactorily high.
However, as with any invasive medical procedure there are inherent risks. Overall, the risk of a major complication from nephrostomy placement is about 2- 5%, with a minor complication rate in the order of 7- 10%. There is an approximately 5% chance that the Radiologist will not be able to place the nephrostomy catheter, or that it may become dislodged.
Those related to this procedure include:
Infection- This can never be completely eliminated. However, the risk is very minimal because of the sterile environment.
Damage to the kidney- The kidney is surrounded by a protective capsule which has to be breached during the procedure. This can cause damage to the structure of the kidney.
Damage to vessels causing haemorrhage- This is potentially the most serious complication. The collecting system is very closely associated with the vessels. The Radiologist deliberately tries to aim for a section of the kidney which has a relatively sparse blood supply.
Pneumothorax- Sometimes it is necessary to enter the skin between the ribs rather than directly below the bottom 12th rib. This increases the risk of puncturing covering of the lung(pleura). This will cause air to escape in and collect between the coverings of lung, is called a pneumothorax. This is usually treated by observation, but if it causes breathing problems then a drain placed into the chest may be necessary.
Damage to other organs- Due to the close proximity of the bowel, spleen and liver.
Urine leak- Urine can escape into the tissues surrounding the kidney. This is usually self limiting.
References
Chalmers N et al. The UK nephrostomy audit. Can a voluntary registry produce robust performance data. Clinical radiology. 2008(63). 888-894.
Making the best use of clinical radiology services. Referral guidelines. 6th edition. Royal College Radiologists.
Dyer RB et al. Percutaneous nephrostomy with extension of the technique: step by step. Radiographics. 2002. 22(3): 503-25.
Lee WJ. Emergency percutaneous nephrostomy: results and complications. Journal of Vascular Interventional Radiology. 1994(5). 135-9.
Pollard AJ. Percutaneous nephrostomy: how is it done. Journal of Interventional Radiology. 1994(9):129-41.