Patients
-
- Angiography
- Angioplasty and Stenting
- Aortic Aneurysms
- Biliary Drainage and Stenting
- Carotid Artery Stenting
- Central Venous Access
- Colonic Stenting
- Fibroids
- Gastrointestinal Haemorrhage
- Gastrostomy
- Hepatic Malignancies
- Kidney Tumour Ablation
- Minimally Invasive Treatments for Vascular Disease
- Nephrostomy
- Oesophageal Stents
- Pelvic Venous Congestion Syndrome
- Percutaneous Nephrolithotomy
- Prostate Artery Embolisation PAE
- Pulmonary Arteriovenous Malformations
- PAE Patient Information Leaflet
- Ureteric Stenting
- Varicoceles
- Varicose Veins
- Vascular Malformations
- Vertebral Compression Fractures
- Vertebroplasty and Kyphoplasty
Colonic Stenting
Content by - Dr. D. Kusumawidjaja and Dr. R.S.Kasthuri
What is a colonic (large bowel) stent?
A colonic stent is a hallow cylindrical tube, usually made of metal or an alloy which helps to keep the lumen of the large bowel open. (Figures.1&2).
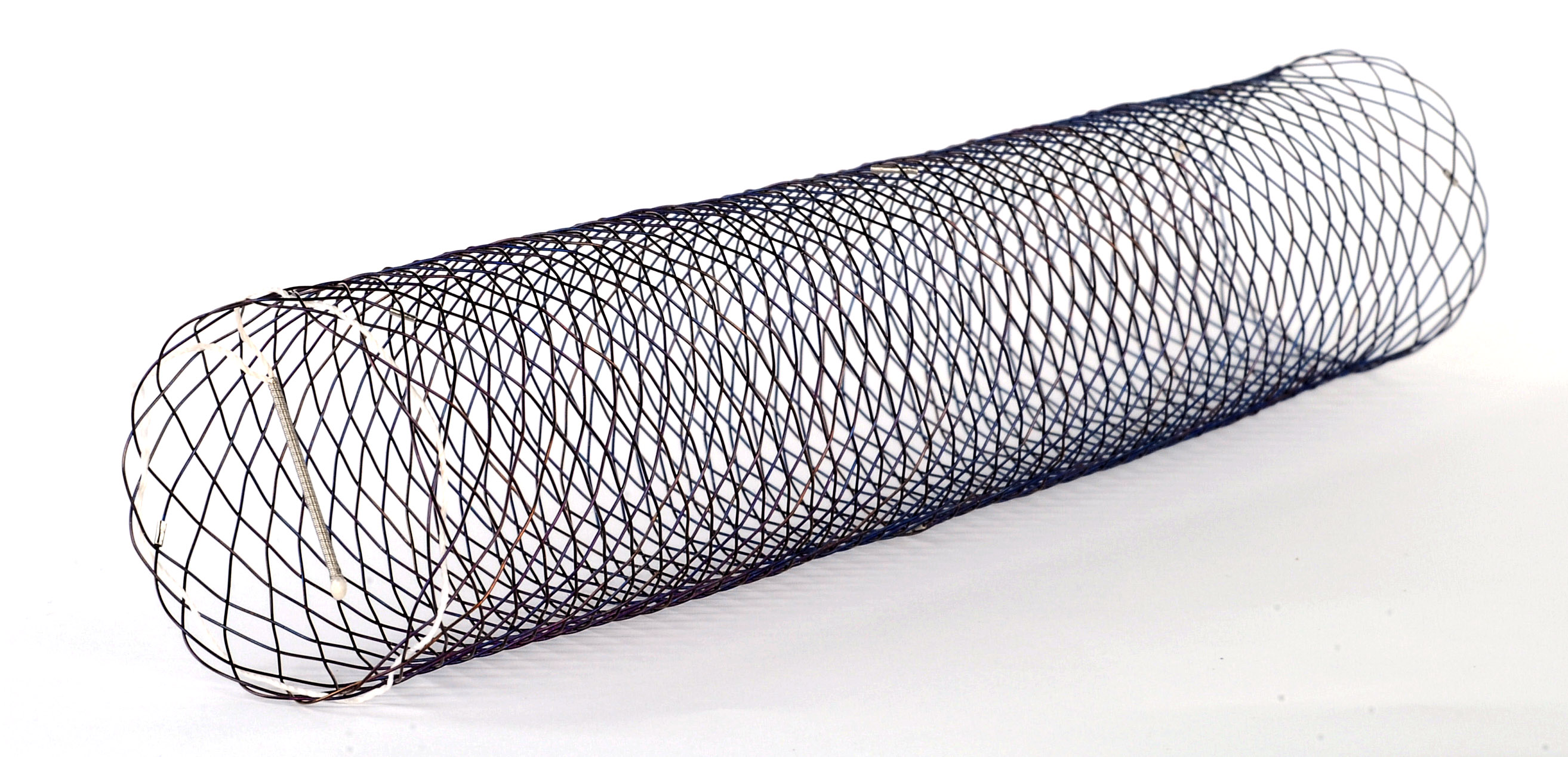
Figure 1. Picture of a colonic stent
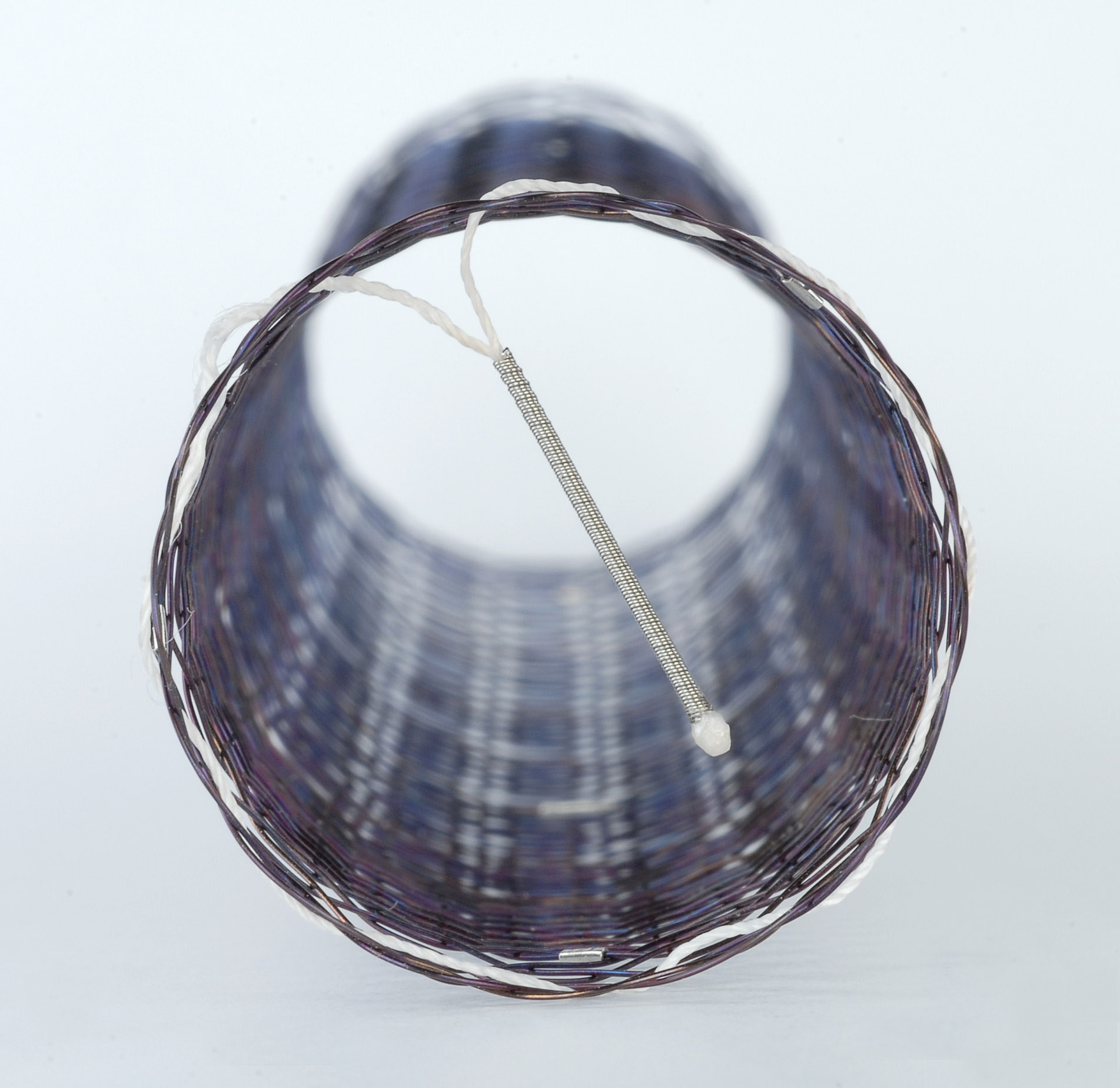
Figure 2. Picture of a colonic stent
When is a colonic stent used?
A colonic stent is used to relieve complete or partial large bowel blockage.
How does the colonic stent work?
The stent is compressed tightly onto a small delivery wire which allows the stent to be positioned across the tight narrowing which has caused the blockage. Once opened, it relieves the obstruction by keeping the colon open. It can take up to 24 hours for the stent to fully open. (Figures.3-5)

Figure 3. X-ray image of a blocked lower large bowel
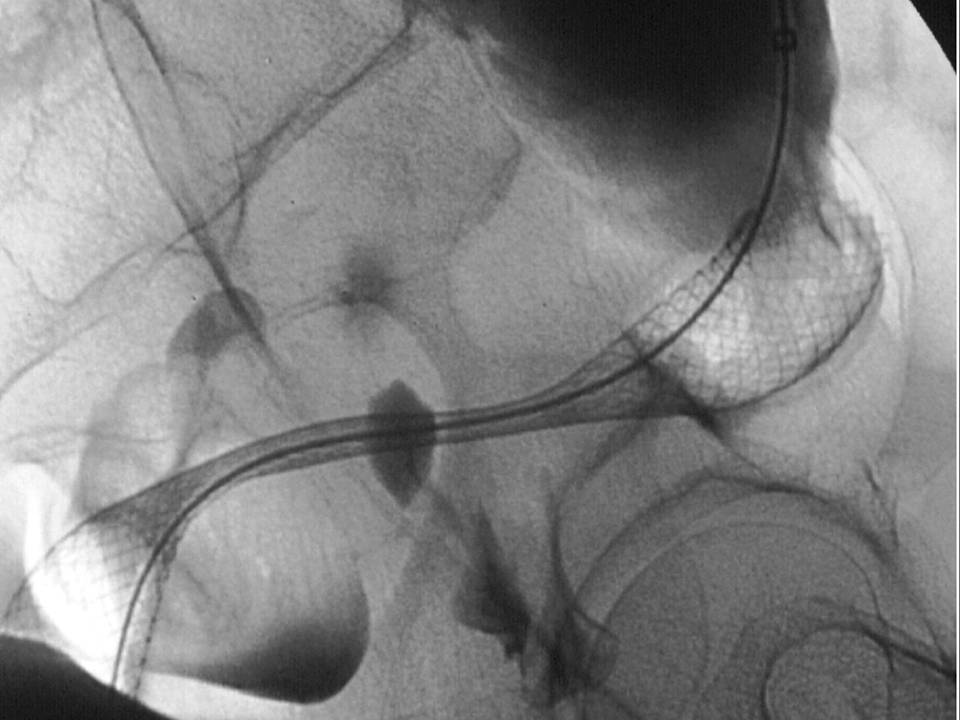
Figure 4. X-ray image of a colonic stent in place
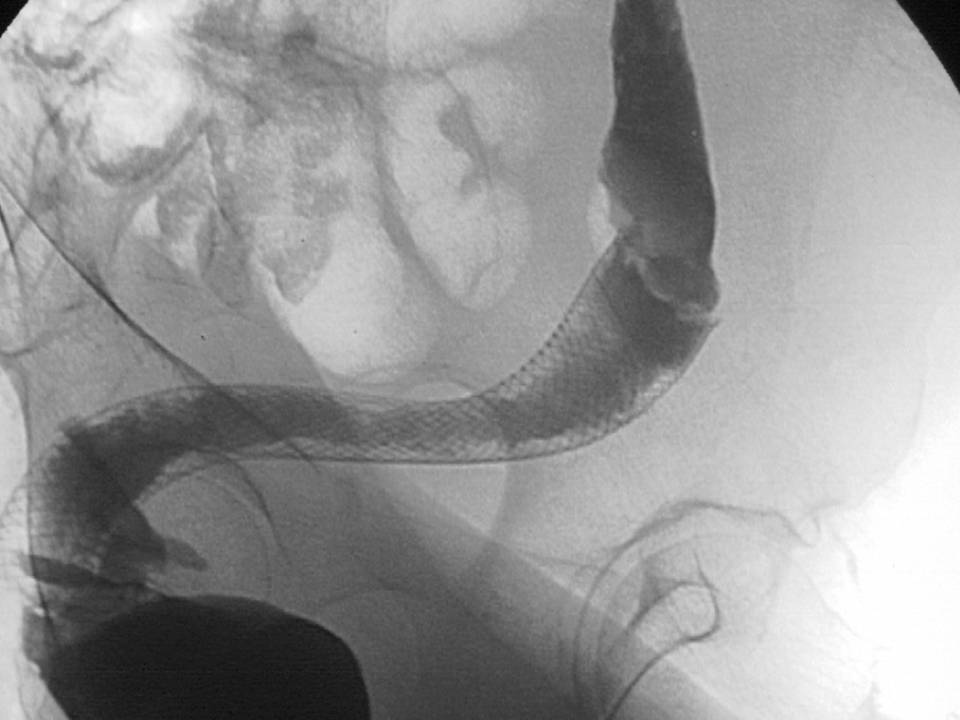
Figure 5. X-ray contrast dye demonstrating the previously blocked bowel to be deflated
Who performs colonic stenting?
Colonic stents are performed by specialist doctors; either by an endoscopist (using a telescopic camera) or by an interventional radiologist (using special X-ray equipment). These are often performed jointly.
Where will this take place?
Colonic stenting is often performed in the X-ray department. This allows the procedure to be visualised and guided by X-rays. Sometimes, it is performed in the endoscopy suite by an endoscopist using a telescopic camera.
Is any preparation required?
No specific preparation is required. The patient is usually an in-patient, admitted in the hospital and will not usually be allowed to eat or drink for 4 hours beforehand.
What will happen to me when it takes place?
The patient is brought down to the X-ray department (or endoscopy suite if an endoscopist is performing the procedure alone). Sedation (medication to make patient sleepy) is usually given during the procedure. Vital signs (such as your pulse rate and breathing) will be monitored throughout the procedure and oxygen to breathe through a tube or mask is usually given.
The patient is placed on a table with X-ray equipment overhead. This equipment may come very close to the body during the procedure. If both an endoscopist and radiologist are performing this, an endoscope (telescopic camera) will first be passed into the back passage before a wire is positioned. The radiologist will pass the stent along this wire before releasing it in place.
How long will it take?
It is difficult to predict this as every case is different. Straightforward cases take about 30-40 minutes and the more difficult ones take longer.
What are the alternatives?
The alternative to colonic stenting is an operation. Usually involves bringing the bowel to the skin and a stoma (A bag on the skin into which the bowel empties).
Sometimes, the colonic stenting procedure is followed by an operation.
The patient should speak to the team looking after them to discuss potential options. There are usually detailed discussions between the radiologists and the clinical team.
What are the complications?
This procedure is usually very safe and there are few risks.
Sometimes, it will not be possible to position the stent in a safe position and the procedure may have to be abandoned. If this happens, alternatives will be considered.
The patient may experience some pain during the procedure and for a short time afterwards as the stent expands to its fully formed shape.
Small amount of bleeding is not uncommon, but this settles. Large amount of bleeding should be highlighted to the clinical team.
Other complications are rare; these include stent migration (movement), stent failure and bowel perforation (hole in the bowel).
- Stent migration is when the stent moves out of its intended position.
- Stent failure occurs when the stent becomes ineffective either because it had not become fully released or if there has been disease progression. If any of this happens, your doctor may decide that a further attempt at stenting may be necessary.
- Bowel perforation is very rare (less than 5%) and may happen either at the time of the procedure or at a later time. In the unlikely event that bowel perforation has occurred, you may require an operation to fix this.
Are there NICE guidelines for colonic stenting?
The national institute of health and clinical excellence (NICE) was notified in April 2002. NICE has classified colonic stenting as an established procedure with sufficiently known safety profile. Therefore there is no requirement for guidelines.
Is colonic stenting performed in the private sector?
Yes. Most hospitals in the private sector are able offer colonic stenting, but local practices vary. You should contact a local private hospital for more details.