Clinical Practice Guidelines

Duty of Candour Statement
2025 Update

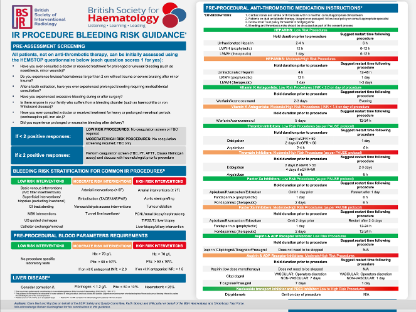
IR Bleeding Risk Guidance
2025 Update

BSIR Library
View guidance, statements and documents.
Charity Info
British Society of Interventional Radiology (BSIR)
The Royal College of Radiologists
63 Lincoln’s Inn Fields
London WC2A 3JW