-
Members
- BSIR Elections
- BSIR Bursaries, Awards and Grants
- BSIR Mentoring Scheme
- BSIR Honorary Awards Open Nominations Process
- Learning Zone
- Vacancies
- BSIR Executive Officers and Committee Reports and Meetings
- Society General Information
- BSIR Society and Special Interest Newsletters
- National Clinical Impact Awards
Developing Day Case Units - Imperative for Optimal Patient Care in Interventional Radiology
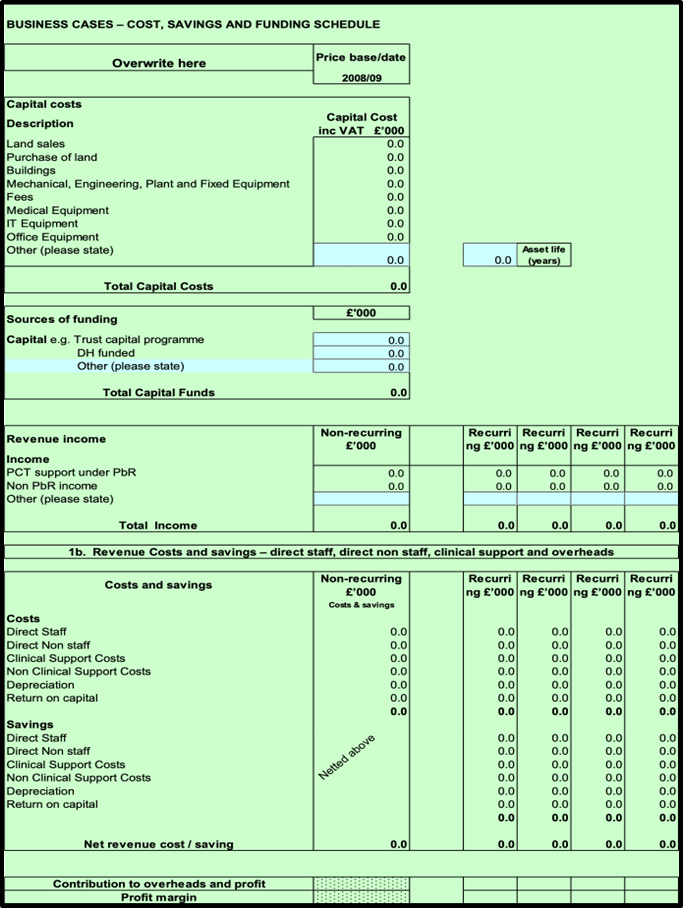
PLEASE SEE BELOW AN EXAMPLE OF A BUSINESS CASE TEMPLATE. IF YOU WISH TO SAVE THIS, IT IS AVAILABLE TO DOWNLOAD AT THE BOTTOM OF THE PAGE, YOU CAN ALSO SAVE TO YOUR BSIR LOCKER AS A RESOURCE.
Business Case Template
|
IR DAY CASE UNIT (*please alter/transpose onto local Trust document) |
|
Business Case Originator / Lead Contact: |
|
General Manager: |
|
|
Directorate: |
RADIOLOGY |
Ref: |
|
|
Review Panel Authorisation: |
|
||
|
1. Exec Summary Exec summary should be limited to half page max, Further background detail should be provided in Section 8: Background to proposal. Please be clear about specifically what this proposal is requesting. This business case document has been prepared to propose the development of a dedicated Interventional Radiology (IR) daycase unit - to be located in the *** (complete as necessary) at *** (complete as necessary) Trust, with the aim to release capacity in the *Surgical Day Unit (SDM) or *Inpatient Wards (*delete as appropriate), which is a Trust priority. It will also improve patient flow and increase efficiency for the IR service. (N.B. If part of a phased development, list the phased stages with supporting evidence in the Appendix clearly outlining overall strategy.) An IR daycase unit will deliver the following core benefits to the Trust:
Due to the minimally invasive nature of image guided IR procedures, procedures are commonly performed under local anaesthesia and consequently, patients recover rapidly with over 90% of procedures requiring day case admission only. Reconfiguration of IR services through a dedicated IR daycase unit is vital to ensure best medical practice in line with the GIRFT National Day Surgery Delivery Pack (Link: https://www.gettingitrightfirsttime.co.uk/wp-content/uploads/2021/08/National-Day-Surgery-Delivery-Pack_Aug2021_final.pdf).
If requesting funding from Charity please also complete Section 5 |
|
2. Financial Headlines: Briefly outline key costs, net surplus / loss and source(s) of funding To deliver this service development, we will require capital costs totaling £*** and revenue pay costs of £*** k for the increased staff detailed in Appendix *** – ‘Workforce’. Additional funds for £*** of ward consumables and £*** for IT will also be required. Full summary breakdown in table format included in Section 3. Daycase service provision is well established at *** (complete as necessary) evidence based by excellence in clinical outcomes, efficiencies and financial savings as demonstrated by existing Surgery and Endoscopy Daycase Units. (*Liaise with Day Surgery Unit/Endoscopy - ask for any audit data they can share to support the application). Please see the funding summary sourced from alternative hospital sites (*Contact SUHT/East Midlands who have recently had successful applications accepted if required). |
|
3. Estimate Resource Implications |
|||||
|
Capital & Non recurrent Costs £k |
Income (per annum) £k |
Recurrent & Non-Recurrent Costs (per annum) £k |
|||
|
Building* ex. VAT |
|
PBR |
|
Recurrent Costs (per annum) |
|
|
Building* inc. VAT |
|
Non-PBR income |
|
Staff |
|
|
|
|
Other |
|
Non-staff (inc. VAT) |
|
|
|
|
|
|
Clinical Support |
|
|
|
|
|
|
Non-clinical support (inc. VAT) |
|
|
|
|
|
|
Maintenance : Total inc. VAT |
|
|
|
|
|
|
Capital charge (dep + ROC) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Non recurrent revenue costs : |
|
|
|
|
|
|
Staff |
|
|
|
|
|
|
Equipment |
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
Total exc. VAT |
|
|
|
Total Recurrent inc. VAT |
|
|
Total inc. VAT |
|
|
|
Total Non Recurrent inc. VAT |
|
|
4. Net Surplus / Loss
* Note that for Building work, ballpark quotes only are required for the initial concept form submission and ballpark quotes only will be provided by Estates unless business case / concept has already been agreed by Review Panel. |
|||||
|
5. Charity Funding Requests: Not applicable - no charity funding requested OR complete if part of a charitable application.
|
|
6. Type of Business Case (please indicate Y / N as appropriate) |
||||
|
a. Capital Cost: Y |
If Y: Is this on the capital plan: Y / N |
|||
|
b. Revenue Cost: Y |
c. Non recurrent: N |
d. Income: Y |
||
|
e. Invest to Save: Y |
||||
|
f. Quality Bid: Y |
||||
|
g. Risk management: N |
If Y: Risk Register Ref no.: |
Risk Register Score: |
||
|
h. Equipment: Y |
If Y: Is it replacement: N |
If Y is it : “like for like” Y / N or upgrade Y / N |
||
|
For equipment, please ensure that section 20 is completed with info that will be required for MEC/ Purchasing. |
||||
|
7. Has this project been considered for joint working with *** Trust: Not applicable as no IR service at *** Trust or Yes this is a joint business case working in collaboration with ***. |
||||
|
8. Please confirm Directorate General Manager sign off for the paper (insert name): *** |
||||
|
9. Background to Proposal and Rationale for Proposal: Interventional radiology (IR) is a specialty providing life-saving and cost effective services integral to patient care. It has shifted from a procedure based field to a more clinical specialty in which interventional radiologists take primary responsibility for patients. Due to the minimally invasive nature of image guided IR procedures, the majority are performed under local anaesthesia, and as a result patients recover rapidly with over 90% of procedures requiring day case admission only. Reconfiguration of IR services to provide patient care through a dedicated IR daycase unit would:
IR daycase units are now standard practice UK-wide, and have been a prioritised development during COVID learning to a) facilitate and streamline inpatient care pathways and to b) accommodate altered care pathways in an attempt to relieve strain on hospital beds, which has in turn, redirected additional patient inflow to IR from other medical specialties. |
|
Most importantly, in line with the GIRFT National Day Surgery Delivery Pack (Link: https://www.gettingitrightfirsttime.co.uk/wp-content/uploads/2021/08/National-Day-Surgery-Delivery-Pack_Aug2021_final.pdf), day surgery service provision is recognised as a priority due to its benefits for both patients and system-wide efficiencies related to patient quality and experience, reduced waiting times, release of valuable bed stock and significant financial implications. Specifically, best practice recommendations state that the entire daycase service, ‘IR Daycase’ for the purpose of this business case, should be provided in a standalone dedicated unit, discrete from inpatient activity, containing pathways that incorporate the complete day case process (from pre assessment to discharge).
Activity and demand: Projection and forecast analysis estimates a local annual increase of **% for oncological/vascular/embolisation (*audit and complete) referrals due to the innovation and expansion within the IR field globally. This annual increase in IR demand and innovation expansion, needs to be a central focus for streamlining the IR service to ensure referral waits can be managed for now and the future.
To future proof the IR service, and ensure increasing annual capacity is addressed, it is realised that a multifaceted approach has required (which may include options such as weekend working and extended days), however a significant proportion of this demand can be alleviated by service provision through an efficient, streamlined, dedicated IR daycase unit.
Using current proposals for an IR daycase unit with *** beds, opening from *** until ***, predictions suggest the IR daycase unit would enable the team to increase throughput of the patients by *** per day. (*Calculate and insert).
Plans: *Insert here detailed design of plans and requirements. *Possibly include capital funding predictions and any other additional costs (structural surveys/air units/offices/clinic room/staff room etc).
Commercial Strategy: A dedicated IR daycase unit would enable the IR service to participate in more funded patient trials due to increased capacity, which would in turn income generate to support the allocation of increased staff support. |
|
10. Alternative Approaches Considered: (why do we need to take this approach – what alternative to achieving the goals have been considered. Please spell out the consequences relating to each of the alternatives of not implementing the proposal.)
Advantages
Disadvantages
b. Option 2: Recommended per this proposal - PREFERRED OPTION Advantages
Disadvantages
|
|
11. Alternative Approaches Considered: (why do we need to take this approach – what alternative to achieving the goals have been considered. Please spell out the consequences relating to each of the alternatives of not implementing the proposal.) By not offering this service development:
|
|
12. Option Scoring |
Option1 |
Option 2 |
Option 3 |
Option 4 |
|
Description |
Do nothing |
Recommended |
|
|
|
↓ Scoring Criteria (/10) |
||||
|
Criteria 1 |
|
|
|
|
|
Reduce waiting times/RTT |
|
|
|
|
|
|
|
|
|
|
|
Criteria 2 |
|
|
|
|
|
Improve patient experience (GS-PEQ) |
|
|
|
|
|
|
|
|
|
|
|
Criteria 3 |
|
|
|
|
|
Increase IR throughput whilst increasing SDU/inpatient capacity |
|
|
|
|
|
|
|
|
|
|
|
Total |
|
|
|
|
|
13. Quality Impact Assessment on Preferred Option
Area of Quality Description of Quality Impact (list all applicable in each section) Quality Aim (Improve, Maintain, Reduce) Quality Metric Impact if not achieved (1-5) Likelihood of not achieving (1-5) Risk Rating Monitoring Arrangement Patient Experience
Patient Safety
Patient Outcome
Performance
|
|
14. Outcome Measures |
|||
|
Additional Activity |
|
|
|
|
HRG |
Volume |
OPD |
Volume |
|
|
|
New |
|
|
|
|
FUP |
|
|
|
|
|
|
|
|
|
||
|
Key Performance Indicators |
Date(s) Delivered |
||
|
Unplanned overnight admission |
|
||
|
Re-admission rates (including A and E) |
|
||
|
Length of stay |
|
||
|
Post-operative GP visits |
|
||
|
Index procedures |
|
||
|
|
|
||
|
Key Quality Indicators (CQUIN, risk management etc) |
Date(s) Delivered |
||
|
|
|
||
|
|
|
||
|
|
|
||
|
Key Patient Indicators (PROMS, survey results, audit results) |
Date(s) Delivered |
||
|
Satisfaction questionnaire (GS-PEQ) |
|
||
|
|
|
||
|
|
|
||
|
15. Financial commentary: (Additional explanatory comment for the table above. Has purchaser support been sought or agreed?) |
|
16. Timetable: When could the development be implemented? This should include an assessment of procurement time required, capital build etc.) Milestone 1
Milestone 2
Milestone 3 |
|
|
Estimated Project Commencement Date |
Estimated Finance and Performance Committee Date |
|
17. Extent of Purchaser / Commissioner Interest? (Has the purchaser instigated this, are they aware of it)
18 Please indicate extent of patient and public involvement in support of the proposal if applicable. Has any involvement been sought or views obtained from governors and PPI forums? Has the level or public consultation required been determined? |
|
19. Strategic Fit: Please tick (✓) which of the following strategic objectives or quality priorities are supported by this proposal |
|
|
Valuing our Staff - Recognising the contribution of our staff and helping them develop and achieve their potential |
✓ |
|
Improving Quality and Reducing Harm - Focusing on continuous improvement and reduction of waste |
✓ |
|
Strengthening Team Working - Developing and strengthening Team RBCH to deliver safe and compassionate care for our patients and shaping future health care across Dorset |
✓ |
|
Listening to Patients - Ensuring meaningful engagement to improve patient experience |
✓ |
|
Hospital Flow |
✓ |
|
Escalation of the Deteriorating Patient |
|
|
Sepsis |
|
|
20. Impact on support services: Outline any impacts on support services, i.e. portering, housekeeping, other facilities, estates, etc. either during implementation (non-recurrent) or ongoing (recurrent). Is there any impact on support services?
Reduced demand on SDU/inpatient beds and associated clinical staff No requirement for escort nursing No requirement for portering services
Increased demand on housekeeping needs and food services Increased demand on maintenance.
If Y, please provide details of support services agreed:
Further consultation will be required to finalise demand and service provision required once bed numbers confirmed.
Is there any support required from IT? IT hardware and support for access to patient electronic records. If Y, please ensure you have raised an IT Change Request (using the e-form on the E-Forms portal) in advance of submitting this business case.
Projects requiring Facilities support need to have their support agreed prior to submitting the business case; this includes agreeing a figure for any resulting costs. For Facilities please contact the Facilities Deputy Manager.
Please note that it is the responsibility of the Concept Paper Originator to ensure that costs incurred by support services as a result of the project are recorded in Section 3 of this form. All such costs will be charged to the project. |
|
21. Equipment Information: To be completed for all equipment (or other purchasing) proposals: It is the Directorate’s responsibility to ensure that the relevant competency based training has been put in place for the staff that will be using this equipment and that the financial implications of this are included within this submission.
Please note that this bid will not proceed unless you have involved procurement Please attach indicative quotations for equipment, maintenance and consumables c. Total Lifetime cost: Total of capital equipment, plus 5 years maintenance and consumables. £……… NB If equates to over £181k then will require OJEU tender. d. Maintenance costs: Are there any maintenance costs for this proposal: If Y, please ensure these are included in the financial summary table on page 1 Please indicate where the maintenance charges will be funded from: e. Consumables: Are there any consumables costs associated with this equipment If Y; Please include in lifecycle cost. If these costs are incremental costs, please include in financials table on p1. f. Asset life: Number years asset life for the new equipment:…….. Please ensure capital charges are included in the financials summary table on page 1. Note applies to all capital except charity funded. |
|
22. Sustainability Considerations: to be completed for all papers
Please briefly describe how the proposed project will improve/ has taken into account the following considerations: a. Operational: (direct cost savings, reduced material inputs/ waste, reduced utility costs etc.) Reduced demand on SDU/Inpatient Ward beds Reduced demand on hospital inpatient stay days for treatment Reduced demand on anaesthetic pre-assessment service provision b. Social: (increased staff wellbeing, stakeholder relations, promotes health, sustainable food etc.) Closer working between two clinical areas (even when using the same clinical team), IR theatres and an IR daycase unit, will promote continuity of care and a holistic team approach to the patient care pathway - building on the Trusts aim of ‘Strengthening team working’* (*adapt to local strategic aims) Opportunity for staff to get involved in new patient pathways and treatment offering an exciting streamlined service to the *** population. Staff development - the opportunity to learn and develop highly transferable skill sets (recovery and daycase care provision) to diversify the nature of work undertaken, contributing to staff retention by promoting personal development, motivation and enthusiasm Improving patient recovery and quality of life is the key component to ensure optimal patient health and fitness, and mental well-being - thus promoting overall health and welfare c. Brand/ Reputational: (risk management, legislative compliance, increased awareness, Good Corporate Citizenship etc.) Ensures Trust is seen to provide ‘state of the art’ and GIRFT compliant Daycase IR services to a wide patient group, many of whom are still working and physically active - fulfilling the Trusts strategic aim of ‘Improving quality and reducing harm’* (*adapt to local strategic aims) Shows the Trust is listening to patients (large local demand for daycase procedural intervention to allow recovery at home) - offering patient choice, particularly to those who are either still working or do not wish to stay overnight in hospital evidence based by ‘Otte DI. Patients’ perspectives and experiences of day case surgery. J Adv Nursing 1996; 23: 1228-1237’. (*if you have any evidence of this from local audit or PPI work also include) Opportunities to enhance brand reputation through research and collaboration with other centres in proposed multi-centre trials if capacity allows d. Carbon Reduction/ Environmental: (energy efficiency, waste minimisation, travel minimisation etc.)
Day case procedure - minimal travel and reduced energy requirements as overnight stay not required Increasing capacity of IR and continuing the introduction of newer IR innovations for minimally invasive procedures will reduce need for higher energy/waste procedure such as robotic surgery. |
|
23. Equality Impact Assessment: to be completed for all papers except “like for like” equipment. Please note that it is the responsibility of the concept paper originator / project lead to undertake an EIA screening exercise on this project PRIOR to this form being submitted, (unless this is for “like for like” equipment replacement, in which case an EIA is not required). Audits will be undertaken to ensure compliance. |
||
|
|
Yes/No |
Rationale The ‘Rationale’ box must be completed whether the answer is Yes or No |
|
1. Does the proposal affect one group less or more favourably than another on the basis of: |
||
|
N |
|
|
N |
|
|
N |
|
|
N |
|
|
N |
|
|
N |
|
|
N |
|
|
N |
|
|
2. Does this proposal affect an individual’s human rights? |
N |
|
|
3. If you have identified potential discrimination, are the exceptions valid, legal and/or justified? |
N/A |
If you answered “No” to Q3: You must refer this project to the Diversity Committee (email to Catherine Paton, HR Dept). You may still proceed with submitting this business case to the Review Panel and other committees within the business planning process, but any outcome of those committees will be subject to the review by the Diversity Committee. |
British Society of Interventional Radiology (BSIR)
The Royal College of Radiologists
63 Lincoln’s Inn Fields
London WC2A 3JW